All published articles of this journal are available on ScienceDirect.

Trend of Cardiovascular Disease Mortality Due to Air Pollution and Non-optimal Temperature in Iran (1990-2030)
Authors Info & Affiliations
Abstract
Introduction
Air pollution and climate change are one of the fundamental problems of the environment and public health, and are considered as one of the risk factors of cardiovascular diseases. As a developing country, Iran is also facing this dilemma. This study aims to investigate trends in cardiovascular mortality related to air pollutants and non-optimal high and low temperatures in Iran from 1990 to 2021, and to forecast until 2030, separately for the two sex groups.
Material and Methods
The data used in this study were obtained from the Global Burden of Disease (GBD) website, the latest version of which is GBD 2021. For analysis, the geographical distribution was used to describe the age-standardized mortality rate in 2021 for each of Iran's provinces in ArcMap GIS software, and then the join-point regression was used to examine annual trends and changes, and to produce a ten-year forecast.
Results
The findings showed that the average annual changes in the mortality rate of cardiovascular disease due to ambient particulate matter, lead exposure, and low temperature have been decreasing from 1990 to 2021, and only for the non-optimal high temperature, an increasing trend was observed in the last ten years, and the forecast also indicates an increase in cases related to this cause.
Discussion
This study examines trends in cardiovascular mortality in Iran from 1990 to 2021 due to air pollution, lead exposure, and non-optimal temperatures, with projections through 2030. The highest mortality rates are observed in provinces with severe air pollution, intensive use of chemical fertilizers, and extreme climate conditions. While mortality linked to particulate matter and lead exposure has declined, deaths related to high temperatures are increasing, highlighting the urgent need for environmental and climate interventions.
Conclusion
Applying the right policies to control and reduce pollutants can also help reduce the risks posed by climate change and will, of course, have a positive effect on cardiovascular mortality in the coming years.
1. INTRODUCTION
Air pollution and climate change are significant public health issues and the most critical environmental problems humanity faces (Wang et al., 2021). According to the World Health Organization (WHO), 1.4 billion people live in areas where air pollutant concentrations exceed WHO's recommended levels (Dehghani et al., 2022). The increasing trend of air pollution in large cities, particularly in developing countries, seriously threatens the health of residents (Dhimal et al., 2021).
Epidemiological, clinical, and toxicological studies have demonstrated a relationship between air pollution and health, with potential impacts including increased mortality and hospital admissions, especially among cardiovascular and respiratory patients (Motairek et al., 2023; Rehman and Rehman, 2022). Cardiovascular Diseases (CVDs) are significant causes of mortality and high healthcare costs worldwide, with rates increasing in recent years. At the beginning of the 20th century, approximately 10% of all deaths were due to CVDs, but this figure has risen to about 50% in developed countries and 25% in developing countries in the 21st century. The increasing prevalence of primary risk factors, including unhealthy lifestyles and air pollution, has driven this growth. Long-term exposure to environmental pollutants can be unavoidable for various reasons, including occupational hazards, fossil fuels, ambient particulate matter, and factories (Hertzog et al., 2024; Hystad et al., 2020). According to a 2017 WHO report, about 72% of deaths due to outdoor air pollution were related to ischemic heart disease and stroke, 14% to lung cancer, and 14% to Chronic Obstructive Pulmonary Disease (COPD) and asthma or acute respiratory infections. This report identifies air pollution as the leading environmental cause of death (Santos et al., 2021).
One of the primary air pollutants is particulate matter, with studies indicating that particles less than 2.5 microns (PM2.5) and less than 10 microns (PM10) are among the primary pollutants linked to cardiovascular disease (Zhang and Routledge, 2020; Chen et al., 2021). In a study by Lina Wang and colleagues, which examined the global distribution and temporal changes in the burden of ischemic heart disease associated with PM2.5 particles from 1990 to 2017, it was shown that in 2017, approximately 977,140 deaths and 21 million Disability-Adjusted Life Years (DALYs) due to ischemic heart disease were attributed to PM2.5 globally. The highest burden was observed in countries with low and medium Social-Demographic Indices (SDI) in Asia, Oceania, and South Africa (Hystad et al., 2020).
Moreover, climate change has led to significant fluctuations in ambient temperature extremes and increased mortality rates. Human activities, particularly urbanization and industrial development, have contributed to increased greenhouse gas emissions and global warming. Greenhouse gas emissions arise from multiple sources, including vehicles, especially motor vehicles, industrial activities, and even indoor air quality in residential buildings, with vehicles as the predominant contributor. As a result, the average global temperature rose by approximately 1.1 °C between 2011 and 2020, placing a substantial proportion of the population at risk of exposure to extreme heat and, more generally, to non-optimal temperature conditions. Non-optimal temperature is defined as ambient temperatures above or below the minimum mortality threshold and has been linked to adverse health effects and elevated mortality risk (Hundessa et al., 2024). Recent Global Burden of Disease studies have identified non-optimal temperature as one of the main risk factors for mortality worldwide. These studies also showed that low and high ambient temperatures contribute to mortality among cardiovascular patients. Additionally, the combination of non-optimal temperatures with population growth and aging has led to increased adverse health outcomes, particularly in CVD patients (Alahmad et al., 2023; Al-Kindi et al., 2023).
Given the rise of industrial cities, climate and environmental changes, global warming, recurrent droughts, sandstorms, and numerous wars worldwide, it is expected that environmental pollutants will increase, consequently having adverse effects on human health. Therefore, in recent decades, numerous studies have examined the effects of air pollution and climate change on health and the incidence of various diseases, such as ocular, respiratory, and cardiovascular diseases, various cancers, and related mortality (Yin et al., 2020).
This study aims to provide a comprehensive assessment of cardiovascular mortality due to air pollutants, including particulate matter pollution, lead exposure, and non-optimal ambient temperatures (high and low) in Iran over 32 years (1990 to 2021). Particulate matter pollution focuses on PM2.5 and PM10. Lead exposure is measured as micrograms of lead per deciliter of blood, and high/low temperature is defined as a daily mean temperature warmer/colder than the TMREL, the temperature with the minimum mortality for all included causes. The population-weighted mean TMREL is 25·6°C, with a range of 21·3–26·6°C.
The study also examines the geographical distribution and trends of these mortality rates for each pollutant, separately for men and women.
2. MATERIALS AND METHODS
2.1. Data
The data used in this study were obtained from the Global Burden of Disease (GBD) website, the latest version of which, GBD2021, is freely accessible to all researchers. (https://vizhub.healthdata.org/gbd-results/).
2.2. Statistical Analysis
The spatial distribution and clustering of CVD mortality rates were assessed using Moran's I and Getis-Ord Gi* statistics to identify spatial autocorrelation between provinces. Moran's I range from +1 (perfect positive spatial autocorrelation or clustering) to -1 (perfect negative spatial autocorrelation or dispersion), with 0 indicating no spatial autocorrelation. The lowest mortality rates were observed in the first quarter, while the highest rates were observed in the fourth quarter. The spatial distribution of mortality rates was visualized using ArcMap GIS software version 10.2. A significance level of 0.05 was used for all statistical tests (Soodejani et al., 2019).
Joinpoint regression was used to identify and quantify significant changes in mortality rate trends. All analyses were conducted using Joinpoint version 5.4.0, a trend analysis software developed by the US National Cancer Institute. In this model, annual age-standardized mortality rates and their corresponding Standard Errors (SEs) were used as input data. The Annual Percentage Change (APC) with a 95% confidence interval was calculated for years with trend changes, and the Average Annual Percentage Change (AAPC) was estimated for each gender group. In this model, if yx represents the rate in year x, then logyx=b 0+b1x, where b 0 and b1. These are the regression model coefficients. The percentage change from year x to year x+1 is calculated as follows Eq. (1):

Years with observed trend changes were considered join points, and trend changes between them were analyzed. The significance of trends was determined using the Monte Carlo permutation method (Dragomirescu et al., 2019). Also, the mortality rates for 2025 and 2030 were estimated using the last trend (final segment) from the joinpoint regression (Khorrami et al., 2023).
3. RESULTS
3.1. Geographical Analysis of Cardiovascular Mortality Rates in 2021
The analysis of cardiovascular mortality rates attributable to ambient particulate matter pollution in 2021 revealed significant regional disparities across Iran, highlighting the critical impact of air pollution on public health. Among women, the provinces with the highest rates of cardiovascular mortality were Fars, Kohgiluyeh, Boyer-Ahmad, and Bushehr, with Bushehr province exhibiting the highest rate. For men, similar hot spots were identified in Bushehr, Kohgiluyeh and Boyer-Ahmad provinces, with additional high rates observed in Kerman, Hormozgan, Chaharmahal and Bakhtiari, Khuzestan, and Golestan provinces (Fig. 1A and B).
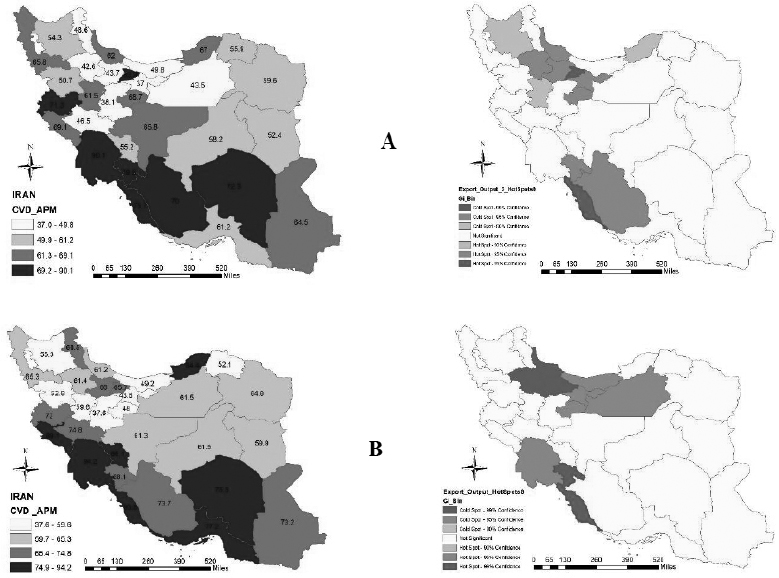
Geographical distribution of cardiovascular mortality rates attributable to ambient particulate matter pollution in Iran, 2021 (A: Women, B: Men).
In both women and men, the provinces of West Azerbaijan, Ilam, and Golestan exhibited the highest cardiovascular mortality rates attributable to lead exposure. Among women, East Azerbaijan, Razavi Khorasan, North Khorasan, and Kermanshah also fell into the highest category. Notably, the hot spots indicate significant similarity between Kurdistan and West Azerbaijan provinces, with a 99% confidence level indicating that West Azerbaijan has the highest cardiovascular mortality rate due to lead exposure. For men, the geographical analysis further revealed that Hormozgan, Chaharmahal, Bakhtiari, and Ardabil provinces also had high cardiovascular mortality rates due to lead exposure (Fig. 2A and B).
The cardiovascular mortality rate attributable to low air temperature showed a consistent distribution across all provinces, with no significant clusters forming among women, and no hot or cold spots were observed with more than 95% confidence. However, the highest rates among women were found in Golestan, Gilan, Alborz, East Azerbaijan, West Azerbaijan, Kermanshah, and Khuzestan provinces. Among men, the provinces with the highest rates were Golestan, Gilan, Ardabil, West Azerbaijan, Lorestan, Ilam, and Khuzestan (Fig. 3A and B).
High temperatures were associated with the highest cardiovascular mortality rates in both genders within the provinces of Sistan and Baluchestan, Kerman, Hormozgan, Bushehr, Khuzestan, Ilam, and Qom. In contrast, the lowest rates, including cold spots, were observed in the northwestern provinces, which generally experience lower average temperatures than other regions of the country (Fig. 4A and B).
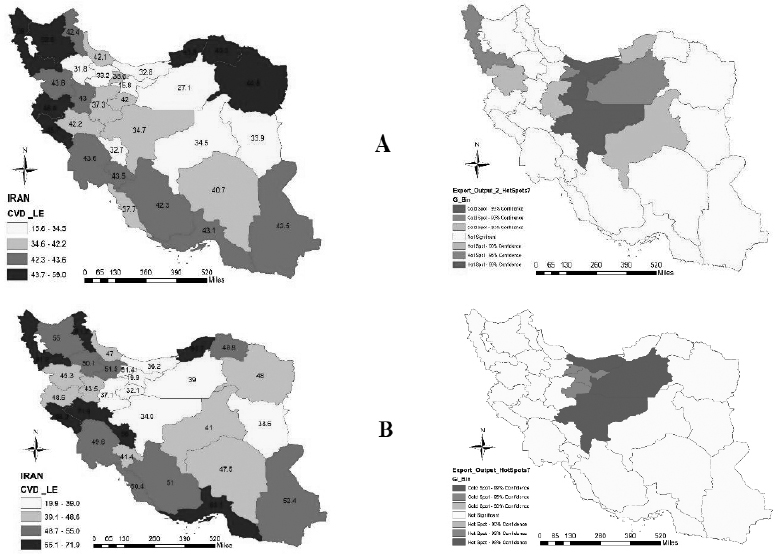
Geographical distribution of cardiovascular mortality rates attributable to lead exposure in Iran, 2021 (A: Women, B: Men).
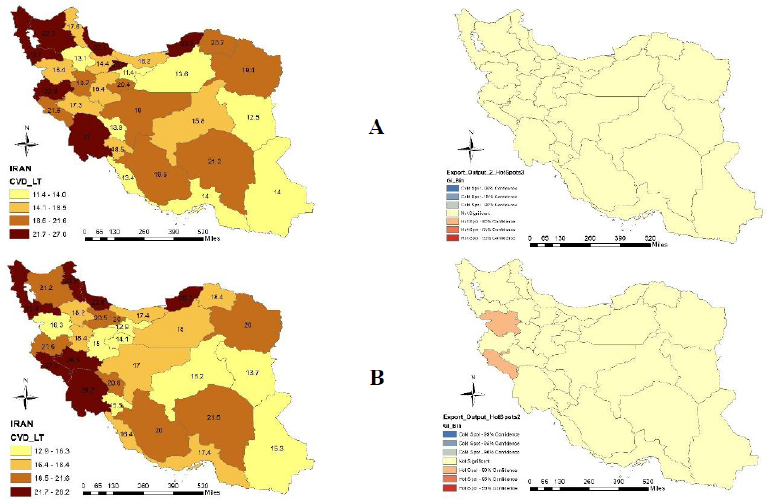
Geographical distribution of cardiovascular mortality rates attributable to low air temperature in Iran, 2021 (A: Women, B: Men).
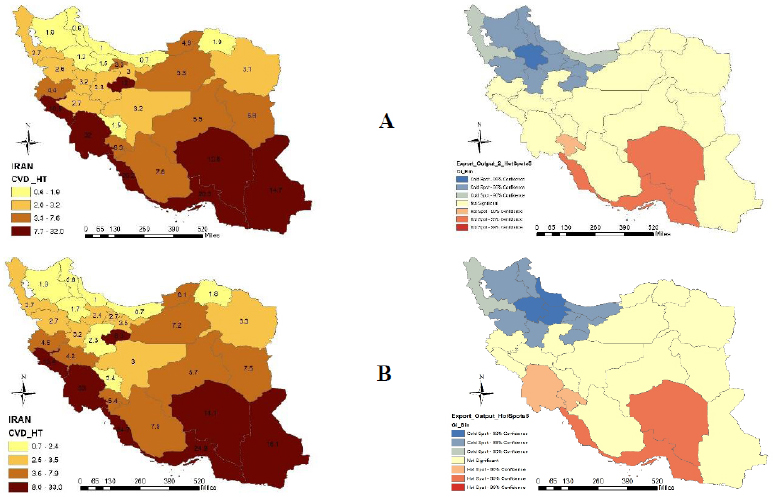
Geographical distribution of cardiovascular mortality rates attributable to high air temperature in Iran, 2021 (A: Women, B: Men).
3.2. Trend Analysis of Cardiovascular Mortality Rates from 1990 to 2021
Trends in cardiovascular mortality rates attributable to ambient particulate matter pollution from 1990 to 2021 reveal significant variation across time segments for both men and women. Among men, the period from 2009 to 2012 showed a notable decline, with an annual percentage change (APC) of -3.51% (p-value = 0.01), indicating a yearly decrease of 3.51% in mortality rates attributable to this pollutant. This decline suggests that measures taken during this period to reduce ambient particulate matter pollution were effective. Similarly, significant trend changes were observed among women from 2001 to 2012, with a decline in mortality rates. Specifically, from 2001 to 2006, there was an annual decrease of 4.44%, followed by a 1.73% decrease from 2006 to 2012. These significant reductions indicate successful efforts to mitigate the impact of this pollutant on public health. Overall, from 1990 to 2021, there was an average annual decrease of 1.77% in cardiovascular mortality attributable to this pollutant among men and 1.62% among women. In the last decade, from 2012 to 2021, the downward trend continued, with a 2.27% decrease in men and a 1.90% decrease in women.
For cardiovascular mortality rates attributable to lead exposure, significant declining trends were observed in men during the periods 1990 to 2000, 2006 to 2012, 2012 to 2018, and 2018 to 2021. The most significant reduction occurred from 2018 to 2021, with an annual decrease of 3.50% in mortality rates. Among women, significant trend changes were observed in all segments except from 2012 to 2017. The most notable decrease occurred from 2002 to 2009, with an annual reduction of 3.07%. The period from 2017 to 2021 also saw a significant decline, with a yearly decrease of 3.01% in mortality rates (Table 1, Figs. (5A-D and 6A-D). The average annual change from 1990 to 2021 also showed a decline, with decreases of 1.65% in men and 1.67% in women. Additionally, during the ten years from 2012 to 2021, there was an average annual reduction of 1.47% in men and 1.45% in women in cardiovascular mortality attributable to lead exposure in Iran, and these changes were significant (Table 2).
Table 1.
| Risk Factor | Male | p-value | Female | p-value | ||
|---|---|---|---|---|---|---|
| Segment | APC (CI 95%) | Segment | APC (CI 95%) | |||
| Ambient particulate matter pollution | 1990-2000 | -0.65 (-1.38, 0.71) | 0.06 | 1990-2001 | -0.03 (-0.22,0.18) | 0.80 |
| 2000-2009 | -1.92 (-2.29, 0.11) | 0.06 | 2001-2006 | -4.44 (-5.46, -3.58) | 0.01 | |
| 2009-2012 | -3.51 (-4.94, -2.94) | 0.01 | 2006-2012 | -1.73 (-3.07, -1.08) | 0.004 | |
| 2012-2016 | -0.37 (-1.68, -1.31) | 0.37 | 2012-2016 | 0.41 (-0.54, 1.40) | 0.25 | |
| 2016-2021 | -3.76 (-0.95, 0.01) | 0.001 | 2016-2021 | -3.71 (-4.40, -3.15) | <0.001 | |
| Lead exposure | 1990-2000 | -1.44 (-3.70, -3.01) | <0.001 | 1990-2002 | -1.05 (-1.14, -0.96) | <0.001 |
| 2000-2006 | -0.06 (-0.95, 0.01) | 0.054 | 2002-2009 | -3.07 (-3.34, -1.29) | <0.001 | |
| 2006-2012 | -3.31 (-3.70, -3.01) | <0.001 | 2009-2012 | -1.49 (-3.01, -0.70) | 0.001 | |
| 2012-2018 | -0.43 (-0.72, -0.01) | 0.04 | 2012-2017 | -0.20 (-0.47, 0.22) | 0.24 | |
| 2018-2021 | -3.50 (-4.53, -2.71) | <0.001 | 2017-2021 | -3.01 (-3.33, -2.69) | <0.001 | |
| High temperature | 1990-1998 | 2.53 (-0.36, 5.51) | 0.08 | 1990-1998 | 3.58 (1.30, 7.68) | 0.001 |
| 1998-2013 | -1.54 (-2.62, -0.46) | 0.007 | 1998-2009 | -3.13 (-9.33, -1.79) | 0.008 | |
| 2013-2021 | 0.60 (-1.75, 3.02) | 0.60 | 2009-2021 | 0.87 (-0.28, 3.65) | 0.14 | |
| Low temperature | 1990-2016 | -2.36 (-2.62, -2.09) | <0.001 | 1990-1992 | 6.23 (-2.01, 13.32) | 0.17 |
| 2016-2019 | 1.61 (-10.26, 15.06) | 0.79 | 1992-2010 | -3.06 (-5.38, -2.68) | 0.01 | |
| 2019-2021 | -7.64 (-19.20, 5.57) | 0.23 | 2010-2021 | -0.08 (-1.78, 0.77) | 0.18 | |
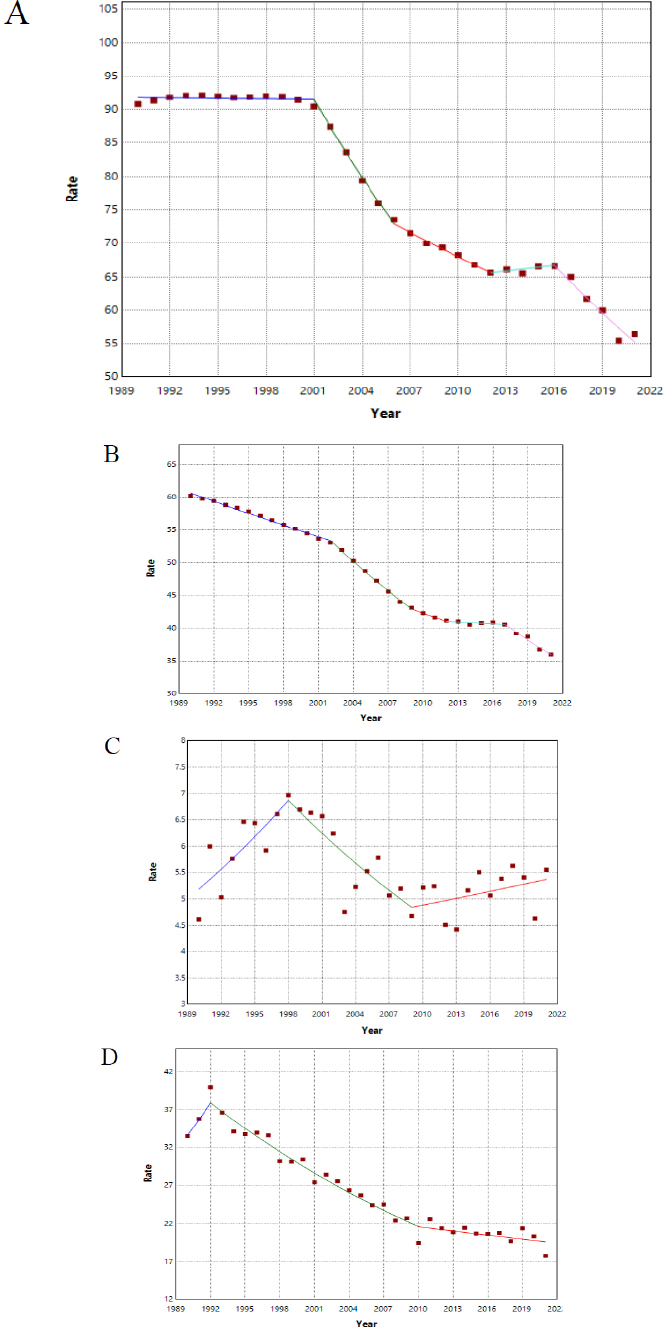
Trends in mortality caused by Air Pollution factors in Iranian women: annual percentage change (A: Ambient particulate matter pollution, B: Lead exposure, C: High temperature, D: Low temperature)
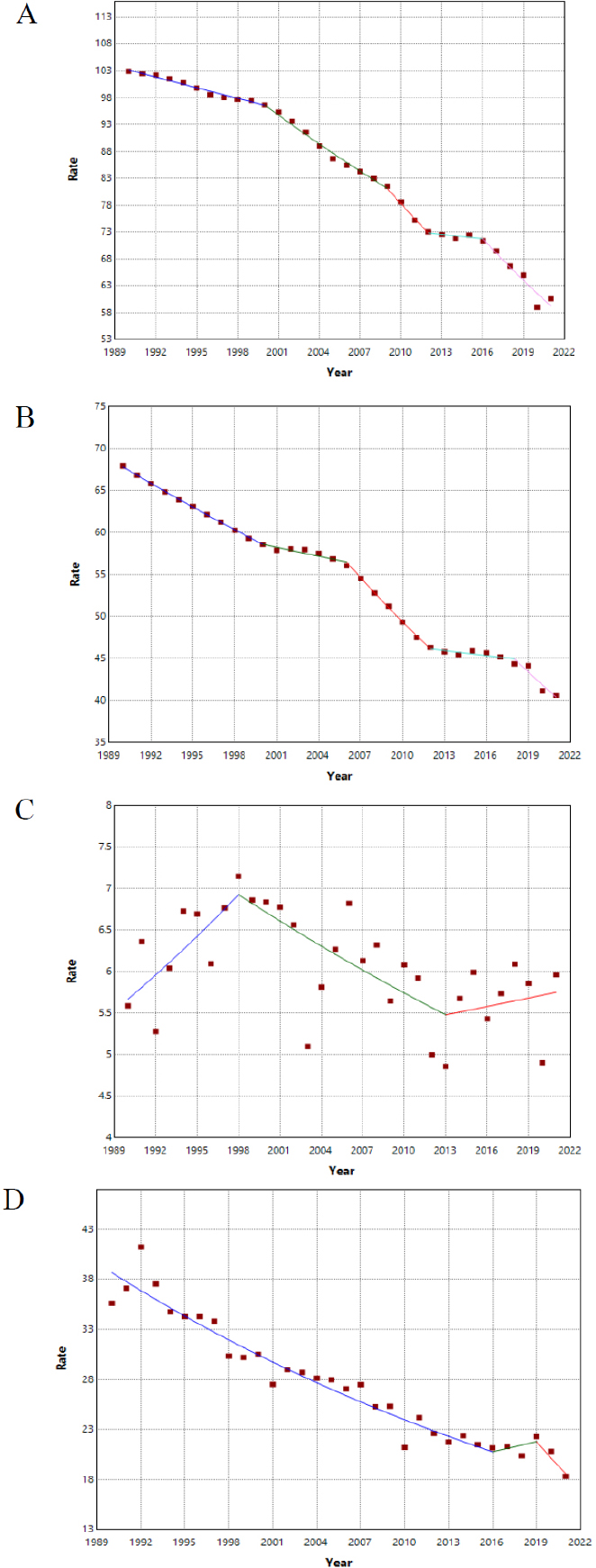
Trends in mortality caused by Air Pollution factors in Iranian men: annual percentage change (A: Ambient particulate matter pollution, B: Lead exposure, C: High temperature, D: Low temperature)
| Risk Factor | Range | Male | Female | ||
|---|---|---|---|---|---|
| AAPC | CI (95%) | AAPC | CI (95%) | ||
| Ambient particulate matter pollution | 1990-2021 | -1.77* | (-1.88, -1.66) | -1.62* | (-1.70, -1.56) |
| 2012-2021 | -2.27* | (-2.74, -1.99) | -1.90* | (-2.23, -1.71) | |
| Lead exposure | 1990-2021 | -1.65* | (-1.71, -1.61) | -1.67* | (-1.70, -1.64) |
| 2012-2021 | -1.47* | (-1.66, -1.31) | -1.45* | (-1.46, -1.60) | |
| High temperature | 1990-2021 | 0.04 | (-0.99, 1.09) | 0.11 | (-0.30, 0.68) |
| 2012-2021 | 0.36 | (-1.63, 2.40) | 0.87 | (-0.28, 2.43) | |
| Low temperature | 1990-2021 | -2.33* | (-3.71, -0.09) | -1.71 | (-2.06, -1.32) |
| 2012-2021 | -2.26 | (-6.89, 2.58) | -0.87 | (-1.72, 0.01) | |
The trend in cardiovascular mortality rates attributable to high temperatures varied across three segments, with some periods showing positive annual percentage changes and others negative ones. Among men, only the trend from 1998 to 2013 was significant, showing a decline in mortality rates due to high temperatures, with a yearly decrease of 1.54% (p-value = 0.007). In women, significant trend changes were observed in the segments from 1990 to 2009, with an annual increase of 3.58% in mortality rates from 1990 to 1998, followed by a yearly decrease of 3.13% in cardiovascular mortality rates due to high temperatures from 1998 to 2009 (Table 1, Figs. 5A-D and 6A-D). Moreover, the average annual changes in mortality rates attributable to high temperatures from 1990 to 2021 and from 2012 to 2021 showed an increasing trend, although this increase was not statistically significant (Table 2).
For cardiovascular mortality rates attributable to low temperatures, the changes from 1990 to 2016 in men were significant, with a decline of 2.36% per year. Among women, significant trend changes were observed from 1992 to 2010, with an annual reduction of 3.06% in cardiovascular mortality rates attributable to low temperatures (Table 1, Figs. 5 and 6).
| Risk Factor | Male | Female | ||
|---|---|---|---|---|
| 2025 | 2030 | 2025 | 2030 | |
| Ambient particulate matter pollution | 51.16 | 42.24 | 47.51 | 39.32 |
| Lead exposure | 35.58 | 29.76 | 31.96 | 27.43 |
| High temperature | 5.20 | 5.35 | 4.76 | 4.97 |
| Low temperature | 16.47 | 11.07 | 19.59 | 18.74 |
Additionally, the average annual changes in mortality rates due to low temperatures from 1990 to 2021 were significant and declining among men, with an annual reduction of 2.33%. However, this decline was not significant among women. Moreover, the average annual changes during the ten years from 2012 to 2021, although downward, were not statistically significant (Table 2).
The predictions based on the final segment in the joinpoint regression also show that the trend until 2030 is ascending only for the non-optimal high temperature, but it is a decrease for the other three risk factors (Table 3).
4. DISCUSSION
With increasing concerns about the adverse effects of air pollution and climate change on human health, a growing number of studies worldwide have reported that air pollution and suboptimal climate conditions are significant environmental contributors to cardiovascular diseases and mortality.
As economic development progresses, accompanied by the increased use of industrial machinery, the rise of factories, emissions from industrial facilities, the use of fossil fuels, and the application of chemical fertilizers in agriculture, environmental pollution has steadily escalated in developing countries like Iran. This pollution has become a serious threat, particularly in large, industrial, and densely populated cities. Moreover, the consequences of climate change have emerged as a significant public health challenge in low- and middle-income countries, including Iran (Alahmad et al., 2023).
Iran, as the second-largest country in the Eastern Mediterranean region of the World Health Organization, is highly vulnerable to climate change and its adverse effects. Recent evidence indicates that Iran has been experiencing reduced rainfall, water scarcity, drought, increased air pollution (especially in industrial cities and densely populated areas), soil erosion, rising temperatures, and an upward trend in natural disasters and mortality related to these climate hazards (Al-Kindi et al., 2023).
This study examines the geographical distribution and trends in cardiovascular mortality attributable to ambient particulate matter, lead exposure, and climate factors, including suboptimal high and low temperatures, from 1990 to 2021, across two gender groups: men and women. The results for each of these pollutants and climate factors are discussed below:
4.1. Ambient Particulate Matter
Exposure to ambient particulate matter is linked to various cardiovascular diseases, including myocardial infarction, arrhythmia, and stroke(Mousavi et al., 2020). The main types of particulate matter associated with respiratory and cardiovascular diseases are PM10 and PM2.5. A study by Rabiei et al. in Isfahan demonstrated a significant association between exposure to PM10 and ischemic heart disease (Dastoorpoor et al., 2021). Similarly, research conducted in the emergency departments of the Respiratory and Cardiovascular Center in Arkansas found that PM2.5 is significantly associated with hypertension and heart failure (Zallaghi et al., 2021).
Numerous studies conducted in Asian countries, including Turkey, China, and Malaysia, have reported significant associations between exposure to heavy metals (such as cadmium, antimony, and arsenic) and air pollutants (such as PM2.5 and PM10) with increased cardiovascular morbidity, disease burden, and related hospital admissions (Abd Rahim et al., 2024, Shi et al., 2024, Ekinci, 2024). For instance, Ekinci et al. demonstrated that each one-unit increase in PM2.5 was associated with a 0.0021 to 0.0029 unit increase in the cardiovascular disease burden (Ekinci, 2024). Similarly, Rahim et al. found that a 10 µg/m3 increase in NO2 concentration was associated with a 7.32% increase in cardiovascular admissions on the day of exposure. Furthermore, elevated PM10 levels showed a significant impact on ischemic heart disease admissions, particularly among patients younger than 65 years (Abd Rahim et al., 2024).
Air pollution from automobile emissions, power plant and factory operations, fires, dust storms, agricultural pollution, and landfills is a major source of these pollutants. The presence of power plants and oil refineries in Bushehr and Khuzestan may contribute to the high cardiovascular mortality rates attributed to ambient particulate matter in these provinces and neighboring regions such as Fars, Hormozgan, Chaharmahal and Bakhtiari, and Kohgiluyeh and Boyer-Ahmad. Additionally, reduced rainfall, dust pollution, and sandstorms in Khuzestan and Kerman increase ambient particulate matter levels, thereby increasing cardiovascular mortality rates.
Provinces such as Kermanshah and Ilam, which also experience high cardiovascular mortality from ambient particulate matter, may be affected by dust transfer from Iraq into western Iran, particularly during spring and summer (Rabiei et al., 2017). In Golestan province, the destruction of pastures and forests due to fires and human activities, the loss of wetlands, and proximity to the desert in Turkmenistan are factors contributing to the high cardiovascular mortality rates associated with ambient particulate matter (Rodopoulou et al., 2015). However, the recent decline in mortality rates suggests that adequate measures have been implemented to reduce ambient particulate matter in Iran.
4.2. Lead Exposure
Lead is a toxic metal with well-documented adverse effects on human health, particularly as a risk factor for cardiovascular diseases. Environmental lead pollution originates from various sources, including industrial activities, agricultural fertilizers and pesticides, and vehicle exhaust (Ghahrchi et al., 2020).
In this study, the highest rates of cardiovascular mortality attributed to lead exposure were observed in the provinces of East Azerbaijan, West Azerbaijan, and Ardabil. This may be linked to the concentration of heavy metals, such as lead, in the Aras River (Khoshnamvand et al., 2021; Shahbazadeh Bengar et al., 2023). Additionally, increased soil erosion and precipitation are directly related to the concentration of heavy metals in river water (Zhang and Wang, 2020).
Golestan province, another region with a high mortality rate due to lead exposure in 2021, has a large agricultural sector. The use of pesticides and chemical fertilizers in this area may contribute significantly to lead pollution. Furthermore, there is a direct relationship among temperature, humidity, and lead concentration, leading to an expected increase in cardiovascular mortality from lead exposure during warmer seasons (Zhang and Wang, 2020; Khraishah et al., 2022).
In North Khorasan and Razavi Khorasan provinces, which have high mortality rates among women, the link may be related to the widespread use of pesticides and chemical fertilizers, as well as industrial and petrochemical activities and mining operations in these areas.
Bushehr province also reported a high mortality rate among men, likely due to the presence of refineries, oil platforms, and industrial activities, with a higher employment rate of men in these sectors compared to women. In western Iran, factors such as refineries, agricultural pesticides, sandstorms, and cement factories may contribute to the elevated cardiovascular mortality rates attributed to lead exposure (Singh, 2022).
However, the observed declining trend in annual mortality rates in recent years suggests that effective measures have been implemented in Iran to reduce the impact of lead exposure on public health.
4.3. Non-optimal High and Low Temperatures
Both high and low environmental temperatures are significantly associated with global mortality. The Global Burden of Disease study estimates that non-optimal temperatures were linked to 1.96 million deaths from various causes worldwide in 2019 (Mumtaz et al., 2022; Hertzog et al., 2024). Cardiovascular mortality, in particular, is associated with both high and low non-optimal temperatures, and countries with lower socio-demographic index values are generally more affected by climate change (Hertzog et al., 2024).
Eighteen countries in the Eastern Mediterranean and the Middle East, with a combined population of approximately 450 million people, are highly vulnerable to climate change. By the end of the century, the region is projected to experience a rise of about 5°C in the average annual temperature, which could have catastrophic consequences. The great diversity of climatic zones, ranging from temperate Mediterranean climates to semi-arid, tropical, and desert regions, highlights the critical importance of climate conditions and temperature variability in the Middle East (Reis et al., 2025).
Exposure to heat increases blood flow to the skin, raises body temperature, and elevates heart rate. Additionally, insensible water loss can lead to hypervolemia and coagulopathy, increasing the risk of myocardial ischemia. Conversely, exposure to cold causes vasoconstriction of the skin to generate and retain heat, which increases blood pressure and the risk of cardiovascular diseases (Hertzog et al., 2024). The results of this study also indicate that provinces with significantly higher or lower average temperatures than the national average, classified as hot or cold regions, exhibit the highest rates of cardiovascular mortality attributable to non-optimal high and low temperatures.
Severe droughts, reduced vegetation cover, soil erosion, along with urban expansion and increased carbon monoxide emissions, may contribute to rising temperatures and adverse environmental changes, which in turn can negatively affect human health. In Iran, southern provinces that have recently experienced recurrent droughts and higher temperatures have also exhibited elevated cardiovascular mortality rates (Ma et al., 2025; Zou et al., 2024).
Furthermore, the annual trend changes reveal an increase in mortality due to high temperatures in recent years, suggesting that the risk of cardiovascular diseases and related mortality is likely to rise as temperatures continue to increase due to climate change. Therefore, it is essential to focus attention on regions with higher average temperatures to mitigate these risks.
As suggestions for future studies, it is recommended that nonlinear models be used and that predictions not be based on the model obtained from the last segment of the trend.
5. STUDY LIMITATION
This study used freely accessible data from the reputable GBD website, which was available up to 2021, and the lack of more recent information is one of the study's limitations. Another limitation is that the rates may not have been adjusted for certain confounding factors.
CONCLUSION
Although air pollution and climate change are now widely recognized as major public health challenges that cause numerous deaths, several policies can significantly mitigate their impacts. Key strategies include improving public transportation infrastructure, implementing emission-control systems for factories, refineries, and other industrial activities, and using appropriate filters to reduce pollution. Additionally, promoting electric vehicles or those with low gasoline and diesel consumption, monitoring factory operations, imposing taxes and fines for excessive pollution, and enforcing environmental regulations are crucial measures.
Enhancing vegetation cover in the southern provinces can help reduce local temperatures and mitigate soil erosion and temperature fluctuations. In provinces where pollutants are likely to contaminate rivers and other water sources, it is recommended to implement proper disinfection measures for plants and pastures exposed to these waters.
Adopting modern agricultural practices, such as reducing the use of chemical fertilizers and pesticides, can also play a vital role in decreasing environmental pollutants. Collectively, these policies would not only improve environmental and climatic conditions but also enhance public health and overall quality of life.
AUTHORS’ CONTRIBUTIONS
The authors confirm contribution to the paper as follows: M.T.S.: Contributed to the conceptualization, study design, data interpretation, and preparation of the first draft; A.A.N.: Responsible for data sorting and collection, participated in the interpretation of results, and contributed to manuscript preparation; V.B.: Contributed to the methodology, statistical analysis, writing, and manuscript preparation; M.M.: Responsible for project administration, study design, statistical analysis, data interpretation, writing, and manuscript preparation. All authors read and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| WHO | = World Health Organization |
| CVDs | = Cardiovascular Diseases |
| SE | = Standard Error |
| APC | = Annual Percentage Change |
| AAPC | = Average Annual Percentage Change |
| GBD | = Global Burden of Disease |
ETHICAL STATEMENT
This research was approved by the ethics committee of Esfarayen Faculty of Medical Sciences, Iran (Ethical Code: IR.ESFARAYENUMS.REC.1403.011).
AVAILABILITY OF DATA AND MATERIALS
The data used in this study were obtained from the Global Burden of Disease (GBD) website, the latest version of which, GBD2021, is freely accessible to all researchers.
ACKNOWLEDGEMENTS
Declared none.
AI DISCLOSURE STATEMENT
During the preparation of this manuscript, the authors used ChatGPT for language editing and grammar improvement. After its use, the authors thoroughly reviewed, verified, and revised all AI-assisted content to ensure accuracy and originality. The authors take full responsibility for the integrity and final content of the published article.

