All published articles of this journal are available on ScienceDirect.

Awareness and Perceptions about Indoor Air Pollution among Health Professional Students: Evidence from a Cross-Sectional Survey from the Northern Emirates of the United Arab Emirates
Authors Info & Affiliations
Abstract
Background
Indoor air pollution is a serious threat to human health, especially for women, children, and adolescents.
Objective
This study aimed to understand the awareness and perceptions about Indoor Air Pollution (IAP) among undergraduate nursing and dental students in the United Arab Emirates.
Methods
A descriptive, cross-sectional survey was conducted on 388 undergraduate nursing and dental students from a health sciences university in the United Arab Emirates. A structured questionnaire was used to collect data. A consecutive sampling technique was used to recruit the study participants. Frequency, percentage, median, and interquartile range were used to summarize the study variables, while Mann Whitney U test and t-test were used to test the differences in statistical significance.
Results
Around 39.7% of the students expressed having somewhat level of knowledge regarding air pollution and its effects (28.4%). Most of the students (54.1%) perceived their indoor air quality to be poor while only 32% were a little worried about it. Of all only 26.3% and 27.8% of the students had a high level of awareness and perception regarding IAP.
Conclusion
The study findings demonstrate an urgent need for strategies like educational campaigns and curriculum redesign to improve air pollution literacy among university students locally and globally.
1. BACKGROUND\INTRODUCTION
Air pollution is becoming one of the challenging environmental problems globally, including in the United Arab Emirates (UAE) and other Middle Eastern countries (Manisalidis et al., 2020; Akasha, Ghaffarpasand and Pope, 2023). Every year, air pollution results in 6.7 million premature deaths globally and of these, 3.2 million deaths are attributed to illness from Indoor Air Pollution (IAP). Improving indoor and outdoor air quality has been one of the UAE government’s aspirations for a long time, as the residents of UAE often spend a significant portion of their time indoors because of high ambient temperatures and cultural factors that may limit outdoor activities (Fawzi Bani Mfarrejet al., 2017). In addition, relative humidity, high temperature, and atmospheric pressure can significantly alter the level of indoor pollutants in the country. There are more than sixty sources of indoor air pollution identified, but these vary from country to country (Salvi and Apte, 2016). The contributors to indoor air pollution in UAE are reported to be from a very broad range of sources, including dampness, mould, cleaning supplies, construction-related chemicals, pesticides, tobacco, and incense smoke, and entrainment from outdoor pollution (Sana Abusinet al., 2022).
Despite being invisible, indoor air pollution can negatively impact the psychological, social, and economic well-being of individuals, society, and nation. IAP is found to be associated with an array of communicable and non-communicable diseases like asthma, acute respiratory infection, chronic obstructive pulmonary disease, lung cancer, tuberculosis, cerebrovascular disease, ischaemic heart disease, low birth weight, and stillbirth with the respiratory system taking the maximum brunt (Salvi and Apte, 2016; Anenberg et al., 2020; Lee et al., 2020; Sana Abusinet al., 2022). As people spend more of their time indoors than outdoors, especially young, older adults, pregnant women, and those with already existing non-communicable diseases, preventing and managing indoor air pollution has become a non-negotiable issue (Franklin et al., 2019).
The most effective way to reduce the hazards from IAP is to minimize the release of pollutants while improving the ventilation and air filtration process. Various simple and low-cost interventions are found to significantly improve the quality of indoor air like increasing the awareness regarding the potential sources, strategies for prevention and mitigation, and how to take care of people who are at increased risk (Ramírez et al., 2019). Healthcare professionals can play a crucial role in educating patients and the public about the dangers of air pollution, strategies to prevent, minimize, and mitigate the associated hazards, and how to take care of people who are at increased risk from IAP. Healthcare professionals can influence the various agencies, leaders, and policymakers at various levels to devise and implement programs to improve indoor air quality. However, it is reported that most of the health professionals’ curricula do not include the health impacts of air pollution, putting future healthcare professionals at risk of not having adequate knowledge and expertise to address people and policymakers about the seriousness of IAP and its associated hazards (Tan, Junghans and Varaden, 2023).
Although a few studies have been conducted to assess the awareness and perception of air pollution among the general public and students, no studies have yet examined the awareness and perception of indoor air pollution among future healthcare professionals. The literature on this topic remains scarce in the context of the United Arab Emirates. Therefore, this study aimed to explore the awareness and perception of indoor air pollution among undergraduate healthcare professional students so that the evidence from the study can be used to provide useful recommendations to the concerned authorities.
2. METHODS
2.1. Study Design, Setting, and Participants
This was a descriptive, cross-sectional study conducted in a selected health sciences University, Ras Al Khaimah, United Arab Emirates, among students enrolled in undergraduate nursing and dental programs in the academic year 2022 to 2023. A consecutive sampling technique was used to recruit the study participants. The data was collected from January to April 2023. Those who were aged above 18 years, and willing to participate were included. No specific exclusion criteria were used. The sample size was estimated using the formula n= [(Z1 -α/2)2 X p X q] /d2. The proportion of awareness about indoor air pollution observed in an earlier publication titled, “Awareness About Indoor Air Pollution in General Population of Rawalpindi and Islamabad,” with a 95% confidence level and 5% relative allowable error, suggests a minimum sample size of 367 (Tariq et al., 2018).
2.2. Data Collection Instruments and Measurement
Data was collected using a structured questionnaire developed by the researchers after reviewing the relevant literature (Lincoln and Eun Hee Kwon, 2017; Lee et al., 2020). Section one collected information regarding the socio-demographic characteristics and living information. Section two included five items to assess participants' perception towards their knowledge of indoor air pollution, indoor air quality at home, perceived risk from IAP, worry of harm caused by/resulting from IAP, and impact of IAP on the health of family members. Section three evaluated the awareness regarding the sources (10 items), health hazards (10 items), and strategies for mitigation (10 items) of IAP using a five-point Likert scale ranging from 1 to 5. The final score of awareness and perception was calculated by adding up the points obtained for the corresponding questions and categorized as high (score ≥80%), moderate (50 – 79%), and low (score < 50%).
The study utilized a validated instrument to improve reliability, thereby minimising the bias. Content validity was ensured by asking 5 experts from nursing and 2 experts from medicine to evaluate the study instrument against a four-point rating scale. They were also asked to comment on the grammatical construction, representativeness, and comprehension. The Content Validity Index (CVI) of the study instrument was found to be 0.84. The instrument also showed satisfactory internal consistency reliability with a Cronbach’s Alpha of 0.89 for the total scale. A pilot testing of the instrument was also conducted to identify issues and no changes were made in the tool thereafter.
A pilot study was also conducted among 30 participants to ensure the feasibility of the actual study. The data collection was carried out using google forms during their free time in the classroom. The survey link was sent via the university email group to the students. A reminder email was also sent after two weeks to maximize the participation of the students. The total response rate for the survey was found to be 93.6% (260+258 =518).
2.3. Ethical Considerations
The study protocol was approved by the research and ethics committee of the institution (RAKMHSU-REC-006-2022/23-F-N, dated 27-10-2022), where the study was conducted. All the eligible participants were given a participant information sheet and consent form along with the questionnaire via google form. Written informed consent was obtained from all the participants before starting the survey. They were informed of their right to withdraw at any time. All data were collected anonymously with no indication of any personal information to encourage honest responses. Explanations about the purpose of the study, the voluntary nature, and the confidentiality of the responses were also assured. Confounding factors were overcome by recording and analyzing pertinent demographic data like age, education, and location.
2.4. Statistical Analysis
Numerical variables were expressed as mean ± SD for parametric variables and Median (IQR) for non-parametric variables. Categorical variables were expressed as frequency and percentage. To compare the mean differences of awareness, perception, and practice with study variables unpaired t-test was applied for parametric data, and Mann Whitney U test was applied for non-parametric data. Chi-square test was used to assess the association of study variables with outcome. Karl Pearson’s correlation coefficient was applied to obtain the correlation among awareness and perception. Data was entered into MS Office Excel and analyzed using statistical software IBM SPSS Version 27. The p-value of 0.05 is considered statistically significant.
3. RESULTS
3.1. Characteristics of Students
The characteristics of students based on the socio-demographic and other living situations are given in Table 1. The majority had neither experienced any symptoms related to air pollution nor their family members were at risk. Most of them had their pets living indoors and had homes with paint peeling. Few (12.9%) had water leaking and odor (8.8%) inside the house.
When asked about their perception of indoor air pollution, most of them reported having a moderate level of knowledge regarding air pollution (39.7%) and its effects (28.4%). Additionally, most students (54.1%) perceived their indoor air quality as poor, with 32% expressing minimal concern about it. Table 2 demonstrates the distribution of students based on their perceptions of indoor air pollution. Only 26.3% and 27.8% of the students had a high level of awareness and perception regarding IAP (Fig. 1, Table 3).
| Variables | Frequency (%) |
|---|---|
| Age in years | |
| < 20 | 210 (54.1) |
| 20-24 | 164 (42.3 |
| >24 | 14 (3.6) |
| Gender | |
| Male | 120.2(31) |
| Female | 267.8(69) |
| Marital status | |
| Single | 368 (94.8) |
| Married | 20 (5.2) |
| Nationality | |
| Emirati | 74 (19.1) |
| Non-Emirati | 314 (80.9) |
| Program Enrolled | |
| Nursing | 250 (64.4) |
| Dental | 138 (35.6) |
| Seminar attended on air pollution | |
| Yes | 54 (13.9) |
| No | 334 (86.1) |
| Living situation | |
| Having family members experiencing symptoms related to IAP | 142 (36.5) |
| Having family members at risk for IAP | 158 (40.7) |
| Having water leaking in the house | 50 (12.9) |
| Having pets living indoors | 100 (25.8) |
| Noticeable odours inside the house | 34 (8.8) |
| Presence of paint peeling in the house | 88 (22.7) |
| Perceived Knowledge Regarding IAP | Frequency (%) |
|---|---|
| Everything | 8 (2.1) |
| Much | 62 (16) |
| Somewhat | 154 (39.7) |
| Little | 132 (34.0) |
| Not at all | 32 (8.2) |
| Perceived indoor air quality at the house | |
| Good | 6 (1.5) |
| Acceptable | 74 (19.1) |
| Poor | 210 (54.1) |
| Very Poor | 98 (25.3) |
| Extent of worry of harm caused by/resulting from IAP | |
| To a great extent | 18 (4.6) |
| Much | 78 (20.1) |
| Somewhat | 86 (22.2) |
| Little | 124 (32.0) |
| None | 82 (21.1) |
| Perceived impact of IAP on the health of family members | |
| To a great extent | 38 (9.8) |
| Much | 96 (24.7) |
| Somewhat | 110 (28.4) |
| Little | 106 (27.3) |
| None | 38 (9.8) |
| Variables |
Completely Agree n (%) |
Agree n (%) |
Neutral n (%) |
Disagree n (%) |
Completely disagree n (%) |
|---|---|---|---|---|---|
| Sources | |||||
| Cooking | 22 (5.7) | 40 (10.3) | 116 (29.9) | 120 (30.9) | 90 (23.2) |
| Smoking | 38 (9.8) | 32 (8.2) | 24 (6.2) | 74 (19.1) | 220 (56.7) |
| Open windows | 34 (8.8) | 44 (11.3) | 146 (37.6) | 106 (27.3) | 58 (14.9) |
| Electrical appliances | 28 (7.2) | 64 (16.5) | 110 (28.4) | 132 (34.0) | 54 (13.9) |
| Refrigerator | 42 (10.8) | 64 (16.5) | 120 (30.9) | 106 (27.3) | 56 (14.4) |
| Pets | 36 (9.3) | 66 (17.0) | 96 (24.7) | 110 (28.4) | 80 (20.6) |
| Gas Heating | 18 (4.6) | 22 (5.7) | 82 (21.1) | 142 (36.6) | 124 (32.0) |
| Carpets | 36 (9.3) | 46 (11.9) | 94 (24.2) | 146 (37.6) | 66 (17.0) |
| Incenses | 32 (8.2) | 64 (16.5) | 98 (25.3) | 120 (30.9) | 74 (19.1) |
| Wallpaper | 40 (10.3) | 62 (16.0) | 104 (26.8) | 112 (28.9) | 70 (18.0) |
| Health consequences | |||||
| Allergy | 16 (4.1) | 8 (2.1) | 58 (14.9) | 124 (32.0) | 182 (46.9) |
| Asthma | 10 (2.6) | 12 (3.1) | 48 (12.4) | 136 (35.1) | 182 (46.9) |
| Cancer | 32 (8.2) | 58 (14.9) | 130 (33.5) | 110 (28.4) | 58 (14.9) |
| Diabetes | 56 (14.4) | 90 (23.2) | 116 (29.9) | 90 (23.2) | 36 (9.3) |
| COPD | 34 (8.8) | 46 (11.9) | 120 (30.9) | 120 (30.9) | 68 (17.5) |
| Lung Cancer | 26 (6.7) | 34 (8.8) | 90 (23.2) | 130 (33.5) | 108 (27.8) |
| Tuberculosis | 22 (5.7) | 48 (12.4) | 100 (25.8) | 120 (30.9) | 98 (25.3) |
| Stroke | 36 (9.3) | 68 (17.5) | 130 (33.5) | 92 (23.7) | 62 (16.0) |
| Epilepsy | 48 (12.4) | 86 (22.2) | 130 (33.5) | 80 (20.6) | 44 (11.3) |
| Autism | 72 (18.6) | 86 (22.2) | 114 (29.4) | 60 (15.5) | 56 (14.4) |
| Strategies for mitigation | |||||
| Installing a range hood | 8 (2.1) | 12 (3.1) | 164 (42.3) | 122 (31.4) | 82 (21.1) |
| Opening windows | 4 (1.0) | 36 (9.3) | 86 (22.2) | 152 (39.2) | 110 (28.4) |
| Closing windows | 42 (10.8) | 62 (16.0) | 136 (35.1) | 90 (23.2) | 58 (14.9) |
| Avoiding/Banning indoor smoking | 16 (4.1) | 10 (2.6) | 46 (11.9) | 98 (25.3) | 218 (56.2) |
| Installing an air quality monitor | 8 (2.1) | 8 (2.1) | 66 (17.0) | 148 (38.1) | 158 (40.7) |
| Regular Cleaning of air filters | 2 (0.5) | 10 (2.6) | 54 (13.9) | 112 (28.9) | 210 (54.1) |
| Regular cleaning of house | 4 (1.0) | 10 (2.6) | 64 (16.5) | 96 (24.7) | 214 (55.2) |
| Regular changing of air filters | 4 (1.0) | 4 (1.0) | 56 (14.4) | 118 (30.4) | 206 (53.1) |
| Using indoor plants | 0 (0.0) | 8 (2.1) | 76 (19.6) | 126 (32.5) | 178 (45.9) |
| Reading labels to check the contents while buying household products | 2 (0.5) | 12 (3.1) | 88 (22.7) | 124 (32.0) | 162 (41.8) |
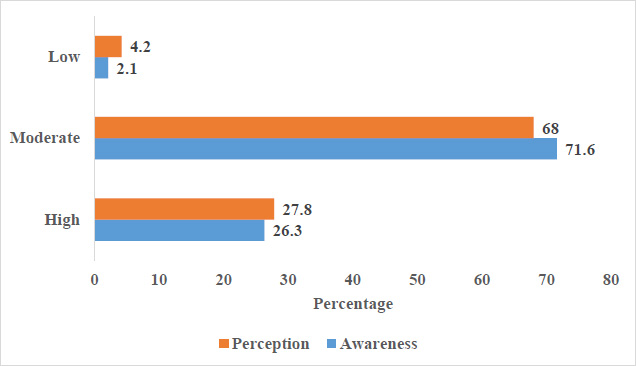
Level of awareness and perception towards indoor air pollution.
Table 4 shows the awareness regarding sources of indoor air pollution among the study participants. It is noted that most of them disagree that cooking, electrical appliances, pets, gas heating, carpets, incense, or wallpaper cause air pollution. More than half (56.7%) completely disagreed that smoking causes indoor air pollution. Most of the participants were of neutral opinion that open windows and refrigerators contribute to air pollution.
4. DISCUSSION
The study revealed significant gaps in awareness and perceptions of Indoor Air Pollution (IAP) among students. While most participants (54.1%) rated their indoor air quality as poor, there was limited awareness and concern about its potential impacts. Awareness regarding major sources such as smoking, cooking, and appliances, and preventative practices like ventilation or air quality monitoring was often underrecognized, indicating a critical knowledge gap suggesting the need for comprehensive educational campaigns, policy initiatives, and behavior change strategies to address these deficiencies.
In the study pertaining to student’s perceptions of risks, it was noted that despite most rating indoor air quality as poor, few participants expressed health concerns. This risk-perception disconnect is seen globally, including in Pakistan, China, and the US(Tariq et al., no date; Raufman et al., 2020; Aguilera et al., 2021). The Health Belief Model posits that low perceived susceptibility prevents engagement in preventive health behaviors, even with exposure awareness (Janz et al., no date). People underestimate personal risks from 'invisible' threats like indoor pollutants. However, clear links exist between indoor pollutants like PM2.5 and adverse respiratory effects (Lee et al., 2020). Targeted educational messaging is imperative to convey health risks, increasing perceived susceptibility.
Most participants in the study did not recognize cooking, smoking, pets, and appliances as pollution sources. However, particulate matter, carbon monoxide, VOCs, and other hazardous emissions from these routine household activities are well documented (Lincoln and Eun Hee Kwon, 2017) This knowledge gap among students mirrors findings in India, Nigeria, and Pakistan (Tariq et al., no date; Afolabi et al., 2016; Ramírez et al., 2019). According to Protection Motivation Theory, threat awareness is a prerequisite for action (Kankaria, Nongkynrih and Gupta, 2014; Lincoln and Eun Hee Kwon, 2017). However, a US study found nursing students frequently used ventilation, contrasting with this UAE study, where participants rarely opened windows/doors and did not support interventions like air monitors or smoking bans (Fawzi Bani Mfarrej et al., 2017). Infrequent cleaning also reflects the low perceived importance of air quality. Lacking literacy of major pollution sources reduces motivation for control. Updated evidence-based training on sources through diverse modalities is vital.
Regarding health impacts, participants disagreed that indoor air pollution causes major respiratory diseases. However, the evidence clearly links indoor air pollution to an increased risk of these diseases. The low awareness contrasts sharply with the well-documented disease burden of household air pollution(Lee et al., 2020).
Awareness regarding IAP was significantly higher among married females and among those having family members experiencing symptoms related to IAP (Table 3). A weak, positive correlation was found between the awareness and perception regarding IAP, as seen in Fig. (2) (p= 0.210, p <0.001).
| Variables | N | Awareness | p value | ||
|---|---|---|---|---|---|
| Mean | SD | Median (IQR) | |||
| Age | |||||
| < 20 | 210 | 110.34 | 16.09 | NA | *0.019 |
| ≥ 20 | 178 | 114.35 | 17.38 | NA | |
| Gender | |||||
| Male | 120 | 108.02 | 16.34 | NA | *0.001 |
| Female | 268 | 114.04 | 16.69 | NA | |
| Marital Status | |||||
| Unmarried | 368 | 111.58 | 16.474 | 110.50 (102.00-122.00) | *0.008 |
| Married | 20 | 123.30 | 19.063 | 126.50 (102.00-135.00) | |
| Nationality | |||||
| Emirati | 74 | 113.54 | 19.442 | 109.00 (101.00-122.25) | 0.791 |
| Non-Emirati | 314 | 111.86 | 16.122 | 112.00 (102.00-122.25) | |
| Program Enrolled | |||||
| Nursing | 250 | 111.03 | 17.638 | NA | 0.070 |
| Dental | 138 | 114.26 | 14.974 | NA | |
| Having Family members experiencing symptoms related to IAP | |||||
| Yes | 142 | 115.06 | 18.089 | NA | *0.010 |
| No | 246 | 110.52 | 15.795 | NA | |
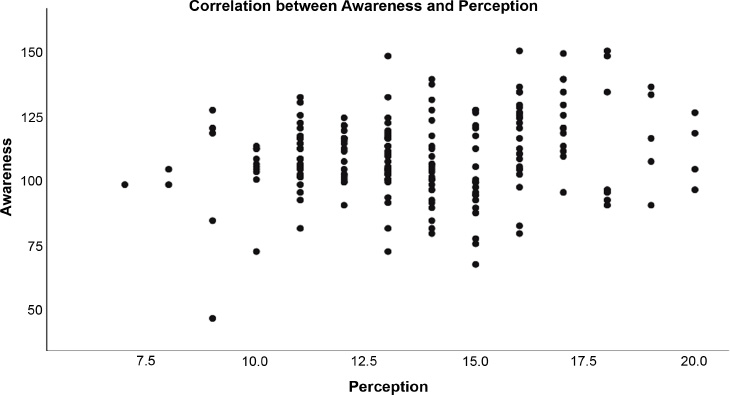
Correlation between awareness and perception regarding IAP.
A systematic review of healthcare students also found low awareness of health consequences, indicating a widespread knowledge gap (Doheny et al., 2023).
In the study, it was also noted that the majority of the participants had a moderate level of awareness regarding IAP. The weather condition in UAE, especially during summer or sand storms forces people to stay indoors. According to a research study, the outdoor particulate matter significantly contributes to indoor air quality in the UAE (Fawzi Bani Mfarrej et al., 2017). Comparable studies also show poor knowledge of sources among university students and the public (Kankaria, Nongkynrih and Gupta, 2014; Joubert, Mantooth and McAllister, 2020; Manisalidis et al., 2020).
Low awareness among future healthcare providers is concerning, given their role in counseling patients and shaping health policies. Reviews show inconsistent air quality education in health professions curricula globally, contributing to knowledge gaps (Kankaria, Nongkynrih and Gupta, 2014; Joubert, Mantooth and McAllister, 2020; Manisalidis et al., 2020). Updated competency-based curricula are essential to convey health impacts.
Statistically significant differences in awareness were found between younger and older students, genders, married status, and family pollution experiences. This aligns with evidence on age, gender, and personal experience effects on health literacy (Kankaria, Nongkynrih and Gupta, 2014; Zhu and Lu, 2023). No program difference agrees with reviews showing inconsistent air quality education in curricula.
Significant differences in awareness by gender and marital status reflect that women and married adults often make efforts to be alert to obtain information and take more health precautions (Fawzi Bani Mfarrej et al., 2017; Ye, Krishnan and Jia, 2022). No age or nationality effects agree with mixed evidence on these factors on awareness or practice (Fawzi Bani Mfarrej et al., 2017; Yu et al., 2018).
Having family members experience health issues related to indoor air pollution was significantly associated with greater awareness in this study. This aligns with the Protection Motivation Theory.Personal experiences increase perceived vulnerability, driving information-seeking and knowledge-building (Fischer-Preßler, Bonaretti and Fischbach, no date). A study in China found that children's respiratory illnesses increased parents' pollution knowledge and risk perception (Zhu and Lu, 2023). However, a US study found no link between children's asthma and adult risk awareness (Black et al., 2017). The mixed evidence highlights that personal experiences may or may not heighten perceived susceptibility and prompt preventive learning. Other factors like health beliefs and coping styles likely mediate responses to illnesses in family members.
The positive correlation found between awareness and perception indicates that improving knowledge is associated with increased risk perception. This aligns with intervention studies showing education programs successfully promoted preventive practices and reduced indoor pollutants (Joubert, Mantooth and McAllister, 2020; Manisalidis et al., 2020; Liu et al., 2023). However, a study in China found no link between knowledge gains and behavior changes, highlighting the complexity of the awareness-practice relationship (Blau, Sela and Grinberg, 2023). The weak correlation coefficient in the current study suggests awareness is not the only driver of risk perception. According to the Health Belief Model, perceived benefits and barriers also shape behaviors (Janz et al., no date; Blau, Sela and Grinberg, 2023). Despite understanding risks, students may see little personal benefit or encounter barriers to recommended practices. Multifaceted interventions using incentives, reminders, social support, and environmental changes are likely needed along with education to maximize behavior change and health impacts.
5. CHALLENGES, OPPORTUNITIES, AND STRATEGIES FOR MITIGATION IAP
Addressing Indoor Air Pollution (IAP) in the study area presents several challenges. Rapid urbanization, industrialization, and construction activities will release various pollutants, which can accumulate in poorly ventilated buildings and spaces. The unique climate and the frequent occurrence of dust storms, cultural practices like incense burning, use of scented cleaning products, and extensive use of air conditioning systems, if not properly maintained, can compromise air indoor quality. Lastly, limited awareness and risk perception can exacerbate the problem, leading to potential health risks for the residents.
Despite these challenges, numerous opportunities are available to enhance the indoor air quality in the Emirate. One is aligning efforts with the UAE’s “Net Zero by 2050” strategy and other sustainability initiatives. Promoting the adoption of clean energy sources and energy-efficient systems, building designs, ventilation practices, and systems, along with educational reforms, presents another opportunity. Integrating air quality modules into curricula can help prepare residents from a younger age and foster institutional awareness of sustainable practices. Additional strategies include implementing dust control measures, enhancing industrial practices, and raising public awareness. Educational campaigns through media, social media, and public health messaging should be implemented to improve awareness of indoor air pollution sources, health risks, and protective behaviors among the general public. These comprehensive approaches can enable Ras Al Khaimah to effectively address its air pollution challenges and foster a healthier environment for its residents.
This study represents a significant contribution to understanding Indoor Air Pollution (IAP) within the context of Ras Al Khaimah, UAE, and among an underserved demographic, undergraduate health professional students. It is among the first investigations in the region to focus explicitly on the awareness and perceptions of IAP among future healthcare providers. The novelty lies in addressing a critical knowledge gap in a setting where students, as prospective health professionals, play a vital role in public health education and policy advocacy. By targeting this demographic, the research establishes a foundation for interventions designed to enhance health literacy and foster leadership in addressing environmental health challenges, particularly in a climate and culture uniquely predisposed to indoor air pollution risks.
6. LIMITATIONS
This study had several limitations, including the use of self-reported data subject to recall and social desirability biases. The cross-sectional single-center design also limits the generalizability of the findings. The study did not evaluate the longitudinal impacts of awareness on practices over time. Perceived versus objectively measured indoor air quality was also not correlated.
7. IMPLICATIONS FOR NURSING PRACTICE
Nurses can provide health education and counsel to patients about indoor air pollution risks, sources, and mitigation strategies. Nurses should exemplify beneficial practices that reduce indoor pollutants in their work settings. They can advocate for institutional and public policies to improve air quality monitoring, building standards, and product regulations. It calls for urgent educational reforms, targeted awareness campaigns, and institutional policies to bridge these gaps and promote sustainable behaviors.
CONCLUSION
Health professionals have an invaluable role in educating communities about air quality risks and prevention strategies. This study revealed suboptimal risk perceptions and knowledge gaps related to indoor air pollution among students. Multipronged strategies are imperative to improve literacy and facilitate healthy behaviors. Targeted educational campaigns, curricular innovations, targeted messaging, monitoring, and robust policy interventions can help address the issues identified. Mass media campaigns, social media engagement, curriculum integration, and indoor air quality monitoring could improve risk awareness and risk perception in this regard.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contribution to the paper as follows: study conception and design: R.K.R., V.E., draft manuscript: P.M., S.P.P. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| IAP | = Indoor Air Pollution |
| CVI | = Content Validity Index |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study protocol was approved by the research and ethics committee of the institution, UAE. (RAKMHSU-REC-006-2022/23-F-N, dated 27-10-2022).
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committees and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Informed written consent was taken from all the participants before enrolling in the study.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article are available within the article.
ACKNOWLEDGEMENTS
The authors are grateful to all the study subjects for their kind participation and cooperation.

